
Psilocybin in End of Life Care
Psilocybin offers promising relief from anxiety, depression, and existential distress in terminally ill patients, with growing research in…

Hospice Volunteers Provide Care, Comfort and Compassion
Hospice volunteers provide essential comfort, companionship, and support, enhancing patient care and offering families peace during end-of-life journeys.

The Power of the Arts in Hospice Care
Discover how music and art therapy bring comfort, connection, and healing to patients in hospice and palliative care,…

The Importance of Geriatric Care Management Services
As we age, our needs evolve. For seniors, these changes may include complex health conditions, mobility issues, or…

Safely Crushing Medications for Hospice Patients
Learn safe methods for crushing medications for hospice patients, including which pills to avoid crushing and alternative options…

I’m In Hospice. Can I Keep My Doctor?
Physician options under the Medicare Hospice Benefit. What is covered, and why many choose to have the personal…
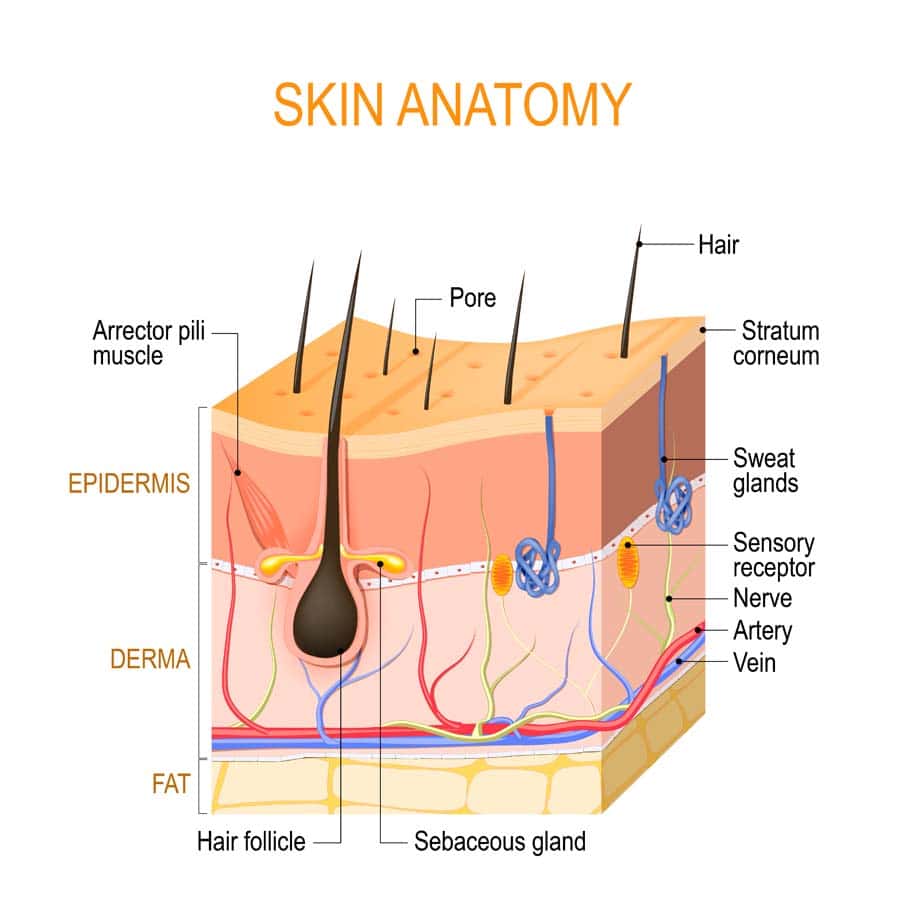
Skin Changes at the End of Life
A comprehensive guide to understanding skin changes at life's end. Learn causes, implications & strategies to alleviate distress…

The Role of Benzodiazepines in Hospice Care
Understanding the role of benzodiazepines for pain relief in hospice care: Benefits, risks, and ethical considerations in managing…



